“Education is not the filling of a pail, but the lighting of afire.”
— William Butler Yeats
When I began my journey into implant dentistry, I was searching for knowledge and purpose—a direction that would guide me toward making a lasting impact in my patients’ lives. The Jacksonville University Comprehensive Oral Implantology Program did far more than provide technical training; it ignited a passion for excellence, empathy, and lifelong learning that will continue to shape every aspect of my career. As a graduate of the program’s inaugural class, I am honored to share my experience and to celebrate a model of education that I believe will transform the future of implant dentistry. As I graduate from the inaugural class of the Jacksonville University Comprehensive Oral Implantology Program, I find myself at a moment of profound reflection—an ending that marks a new beginning. These past 3 years have not only shaped me as a clinician but also deepened my commitment to the field of implant dentistry. I write this editorial to share my journey and shed light on the program that transformed my career. After earning my dental degree in 2020, I felt a strong pull toward oral implantology. I was captivated by the life-changing impact implants can have on patients—restoring both function and confidence with fixed, esthetic solutions. Yet, despite my passion, I struggled to find a structured, comprehensive path-way to truly master this discipline. I pursued countless hours of continuing education across multiple continents. Still, weekend courses, though informative, fell short of the depth and continuity I needed to provide the level of care I aspired to. That all changed when I discovered the newly launched Jacksonville University Comprehensive Oral Implantology Pro-gram. The brainchild of the late Dr. Hilt Tatum—a pioneer whose contributions to implantology are immeasurable—the program was designed for clinicians like myself: those seeking to achieve excellence in all aspects of implant dentistry, surgical, and prosthetics. While traditional specialty programs often divide these components, Dr Tatum envisioned a new kind of training—holistic, patient-centered, and deeply rooted in the principles of NIRISAB (Natural Implant Restoration in Stable Alveolar Bone). Graduates of this program are equipped to manage patientsat any stage of dental handicap, providing them with life-like, esthetic restorations in a safe, efficient, and predictable manner. From initial medical evaluation to final prosthetic delivery, the
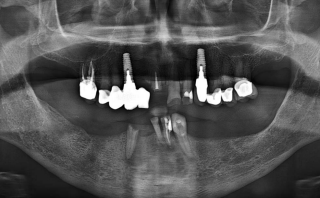
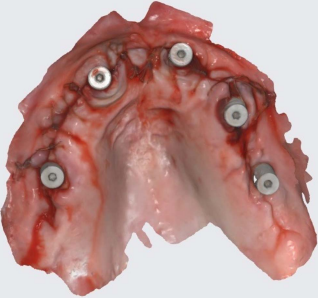
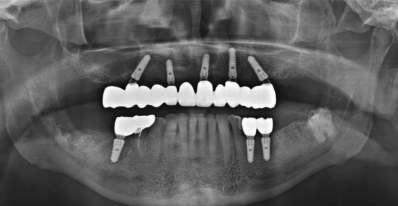
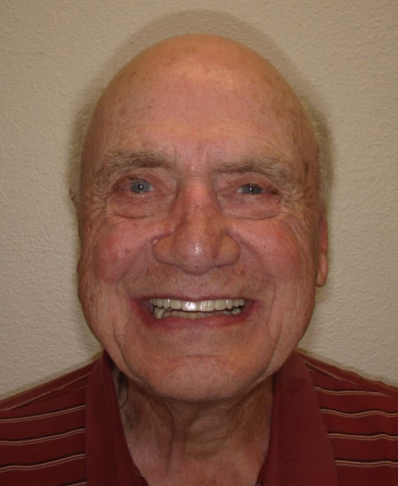
program emphasizes conservative, multidisciplinary treatment planning tailored to each patient’s health, goals, and circumstances. We are trained to educate—rather than persuade—patients, enabling them to make informed decisions they feel confident in. The curriculum also stresses the importance of pre-serving natural dentition whenever possible and integrating implants to harmonize with the patient’s existing oral structures. An essential aspect of our training includes IV sedation and emergency preparedness, ensuring we can safely and comfort-ably treat even the most anxious patients. The didactic component is delivered online and encompasses the full spectrum of implantology—medical evaluation, periodontics, prosthodontics, robotics, remote anchorage, business management, and litigation. Lectures are led by world-renowned implantologists deeply committed to the program’s mission. Each week includes 4 to 5 lectures, reading assignments, and quizzes, culminating in a highlight: the weekly roundtable discussion with Program Director Dr James Rutkowski, whose tireless dedication ensures each student’s success. Clinically, each resident is placed at a partner site, which may be located anywhere in the world. I had the privilege of training at the Brighter Way Institute in Phoenix, Arizona—a nonprofit clinic serving underserved populations, including veterans, those experiencing homelessness, and individuals recovering from addiction. The clinic has state-of-the-art equipment, including intraoral scanners, photogrammetry, a 5-axis mill, and3D printers. Under the guidance of my clinical director, Dr Todd Erickson, I placed and restored nearly 1000 implants. I became proficient in guided and freehand surgeries, advanced bone and soft tissue grafting techniques, sinus lifts, and full-arch rehabilitations using milled PMMA and 3D-printed resin prostheses. A unique feature of my clinical experience was the opportunity to design and fabricate both provisional and final prosthetics. This hands-on approach kept care cost-effective for our patients and sharpened my skills in esthetics, occlusion, and digital design. Perhaps most significantly, every treatment plan was personalized—not a cookie-cutter protocol, but a carefully considered response to each patient’s needs. One patient in particular will always stay with me. He arrived recently released from incarceration, morbidly obese, addicted to cigarettes and soda, and with an extremely high HbA1C. He hoped for dental implants but was far from a suitable surgical candidate. Through patient education and compassionate care, we supported him in making dramatic lifestyle changes. He quit smoking and soda, lost over 100 pounds, and significantly improved his diabetic control. After his transformation, we provided him with a full-arch, screw-retained FP1 prosthesis on the upper and fixed bridges on the lower arch—restoring his smile